A Different Path for Bunion Pain — Without Surgery
Conservative, Non-Surgical Bunion Care — Serving Marble Falls and the Highland Lakes
You’ve probably had your bunion for years — maybe decades. It’s gotten bigger. It’s started to hurt. Shoes don’t fit the way they used to. The second toe may be starting to lean across the first. And somewhere along the way, someone in a white coat told you that the only real fix is surgery.
That’s almost never true. We can’t make a bunion smaller without an operation — but we can almost always relieve your pain, stop the deformity from progressing, and protect you from the cascade of problems that bunions cause when they’re left untreated. For most patients we see, that’s the right answer. And for a small minority who genuinely do need surgery, we tell you that directly.
Medicare and most major insurance plans accepted.

Why I Don’t Recommend Bunion Surgery for Most Patients
What a Bunion Actually Is, and Where It Comes From
A bunion isn’t a bone that grew. It’s a bone that moved.
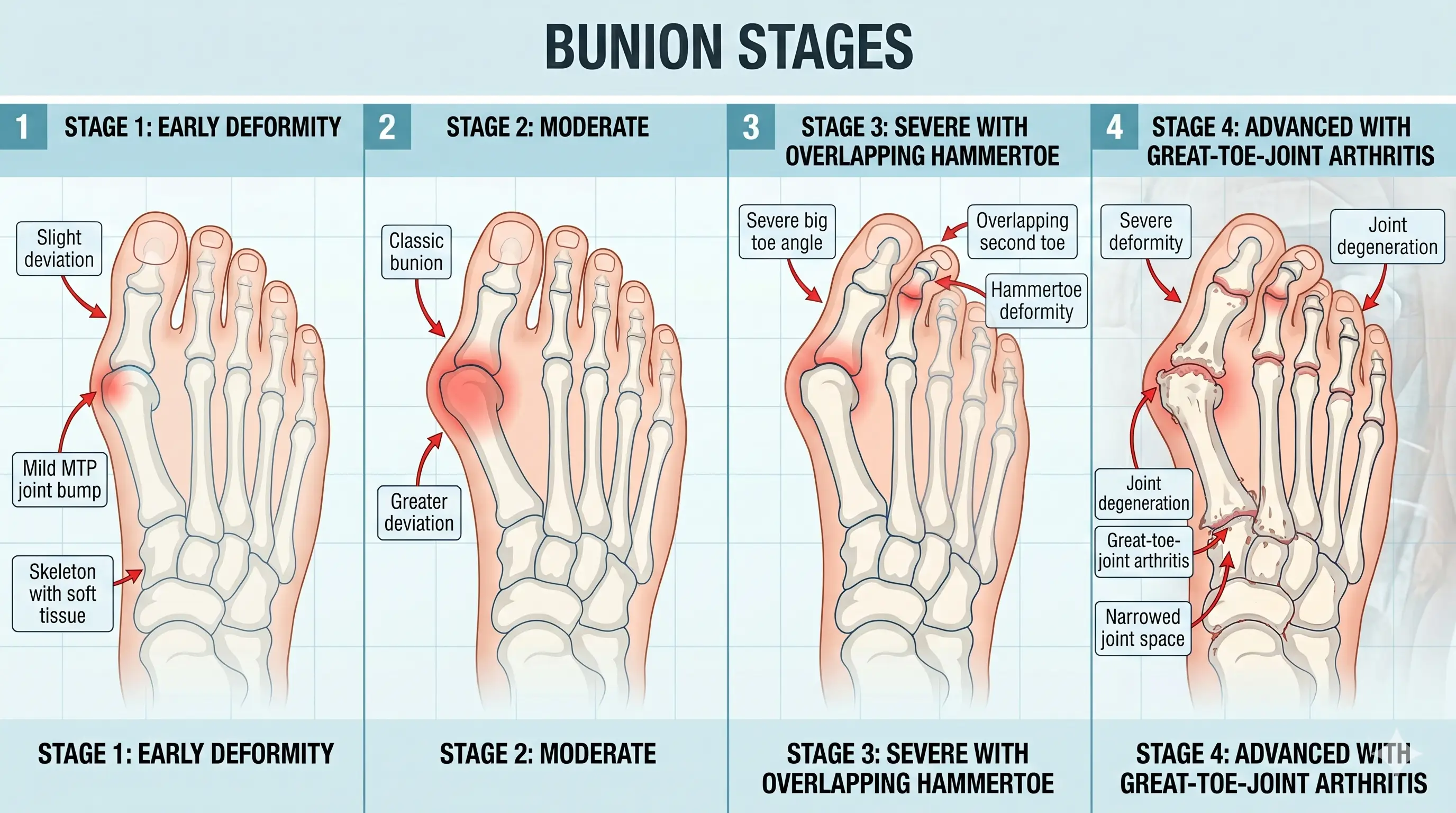
The first metatarsal — the long bone behind your big toe — drifts inward, away from the second metatarsal. The big toe drifts outward, toward the second toe. The joint between them, which used to be a smooth straight hinge, becomes an angled, painful prominence on the inside of your foot. That prominence is what most people call a bunion. It’s also called a hallux valgus deformity in medical literature.
Here’s what’s worth understanding about how you got here:
You weren’t born with a bunion. You were born with a tendency to form one. Bunions are hereditary, but what’s inherited isn’t the bump — it’s the foot mechanics that lead to the bump. If your mother and your sisters all have bunions, that’s because all of you inherited the same underlying foot type: usually a foot that pronates excessively, allowing the first and second metatarsals to spread apart over time.
Bunions usually start forming in the teenage years. They’re slow. Most patients don’t notice anything wrong in their twenties. By the thirties or forties, the deformity is visible. By the fifties or sixties, it often hurts.
Pregnancy accelerates the process — particularly a second pregnancy. This catches most patients off guard. The same hormones that loosen the ligaments of your pelvis to allow childbirth also loosen the ligaments of your feet. After a second pregnancy, the foot itself spreads, pronation increases, and the bunion that was barely there before pregnancy can become significantly worse afterward. This is one of the strongest arguments for wearing prescription orthotics during pregnancy — and almost no obstetrician thinks to mention it.
The big toe joint jams. As the metatarsal drifts inward and the toe drifts outward, the joint stops tracking the way it was designed to. Every step you take is a small impact on a misaligned joint. Over years, that wear accumulates. The joint develops arthritis. The cartilage thins. Bone spurs form. Range of motion is lost. This is the cascade we’re trying to prevent.
The second toe pays the price too. When the big toe leans against the second toe long enough, the second toe can no longer stay in line. It buckles upward into a hammertoe. Eventually it overlaps the great toe. At that point, closed shoes become almost impossible to wear, and surgical correction of the second toe usually requires bunionectomy first — because there’s no room to straighten the second toe until the big toe is moved back out of its way.
This is why treating early matters. The bunion itself is rarely the only problem you’ll have if it’s left alone.
Bunions progress. The earlier we intervene, the more of this cascade we can prevent.
What We Can and Cannot Do Without Surgery
We need to be honest with you about this, because most patients arriving on this page have been told by other doctors that the only “real” treatment is to cut the bone.
We cannot make your bunion smaller. The bone has shifted. We don’t have a non-surgical way to push it back. Toe spacers don’t do it. Bunion splints sold on Amazon don’t do it. Stretching exercises don’t do it. The only way to physically reposition the bone is an operation.
What we can do is far more important. We can:
- Eliminate the pain. In the great majority of patients we see, properly prescribed custom medical orthotics, combined with the right footwear and targeted treatment, resolve the pain entirely.
- Stop the deformity from getting worse. Patients who wear prescription orthotics at least 50% of the time usually halt the progression of their bunion at whatever stage they’re currently in. The bunion you walk in with is generally the bunion you’ll have for the rest of your life — no bigger.
- Prevent the cascade. Properly aligned mechanics protect the great toe joint from accelerating arthritis. They prevent the second toe from being pushed into hammertoe. They preserve your ability to wear closed shoes comfortably.
- Keep you out of the operating room. Most patients we treat for bunions never need surgery. Period.
That’s a much better outcome than most patients realize is available. Surgery treats the bunion; conservative care treats the patient.
A 30-Year Case Study
I want to tell you about my late wife, Sharon.
When we got married, she had small bunions. I made her custom prescription orthotics, and she wore them diligently. After about five years she said she thought the bunions might be getting bigger — like staring at a door in the middle of the night and not being able to tell if it’s actually moving. So we took an X-ray and overlaid it on the films I’d taken five years earlier. There was no change. We did this every five years for thirty years. There was no change.
Over those same thirty years, Sharon’s three sisters — who were so genetically similar that they looked nearly like clones — all developed bunions large enough to require surgery. They all had the surgery. They all had recurrences afterward.
The only difference between Sharon and her sisters was that she wore the orthotics and they didn’t.
I’m not pretending this is a randomized trial. It isn’t. But it’s a clinical observation I made over thirty years of watching the same family, with one variable changed, and the result was clear. It’s why I tell every bunion patient who walks into my office that orthotics — properly prescribed and consistently worn — can stop your bunion’s progression in its tracks.
Why the Things You’ve Already Tried Didn’t Help
If you’ve already been dealing with this for a while, you’ve almost certainly tried one or more of the following. Here’s why they didn’t work — and what it tells us about your bunion.
Toe Spacers and Bunion Splints from Amazon
These don’t fix bunions. They don’t reverse the deformity. They don’t address why the bunion formed in the first place — which is biomechanical. Some patients get modest temporary pain relief from a toe spacer worn alongside an insole, but the relief is coming from the insole, not the spacer. A $20 splint is not a substitute for a proper biomechanical workup.
Wider Shoes
Switching from narrow shoes to wider shoes generally feels better — the bunion no longer rubs as much. But shoes do not cause bunions. They aggravate bunions. Bunions form regardless of footwear: aboriginal populations who have never worn shoes a day in their lives still develop bunions and hammertoes — but they don’t experience the same level of pain we do, because they aren’t wearing shoes that compress an already-misaligned forefoot.
This is also why more women than men end up having bunion surgery. Men aren’t dramatically less prone to bunions. They’re just allowed to wear comfortable shoes and boots that don’t aggravate them. Women have, for generations, been pressured into pointed, narrow, high-heeled fashion shoes that turn a manageable bunion into a painful one. As one of my professors used to say: if the shoe fits — it’s UGLY.
Switching to a wider shoe takes the daily aggravation off your bunion, which matters. But it doesn’t address the mechanics that caused the bunion to form in the first place. The metatarsal continues to drift. The bunion continues to grow. You’ve taken the pressure off the bump without slowing what’s causing it.
Off-the-Shelf Inserts from a Pharmacy or Shoe Store
This is the category most people get wrong, often expensively. A $400 set of inserts from a national arch-support retailer is not a medical orthotic. It’s a comfort product. It cannot control the timing of your gait, the loading pattern of your forefoot, or the positioning of your first ray. If you bought a set and they didn’t help your bunion — that’s not your fault. They were never designed to.
A Cortisone Shot in the Joint
A cortisone shot can quiet down inflammation in an arthritic great toe joint for weeks or months. It does not treat the bunion itself, it does not stop progression, and repeated injections into the same joint can weaken cartilage and worsen the underlying problem over time.
Stretching, Exercises, and Toe Yoga
Strengthening the small muscles of the foot has some benefit and we sometimes recommend it as part of a broader plan. But you cannot exercise your way out of a structural deformity. The bone has moved. Muscle work alone does not move it back.
The reason none of these worked is that none of them addressed the actual cause. We will.
How We Actually Treat Bunions
The Diagnostic Blueprint
Before we treat anything, we look. Weight-bearing digital X-ray to measure your hallux valgus angle, your intermetatarsal angle, and the condition of the great toe joint cartilage. Live diagnostic ultrasound where appropriate. A focused biomechanical examination — foot and ankle range of motion, muscle testing, structural assessment of the first ray. A tape test on the bunion itself, which both gives you immediate diagnostic information about how much pain relief is achievable, and frequently provides immediate symptomatic relief on the day of your visit.
The Mechanical Correction
Custom prescription medical orthotics — built from a precise mold of your foot, engineered with the specific biomechanical corrections your bunion requires. This isn’t a comfort product. It’s a medical device that controls the timing of your gait, supports the first ray, reduces the forces driving your bunion’s progression, and protects the great toe joint from continued wear. With proper care, our orthotics typically last 15–20 years or longer.
The Pain and Inflammation Tools
Where appropriate, advanced injection therapy targeting inflammation in the joint capsule and surrounding tissue. Therapeutic taping protocols to confirm and extend the effect of orthotic correction. Targeted footwear guidance — including which specific brands, lasts, and toe boxes work for your foot type, and which to avoid. Activity modification when needed. Dr. Henry will tell you what’s worth your time and what isn’t, and won’t sell you anything that isn’t part of your specific plan.
“You’ll need orthotics after bunion surgery. Why not wear them first — and skip the surgery altogether?”
— Dr. Frank J. Henry, DPM, FACFASAbout Dr. Henry
Dr. Frank J. Henry has practiced podiatric medicine since 1980 and has been board-certified by the American Board of Foot and Ankle Surgery since 1990 — with full unrestricted scope across the forefoot, rearfoot, and ankle. He studied biomechanics directly under Drs. Root, Weed, Orien, and Sgarlato — the founders of the modern field of foot and ankle biomechanics. In over forty years of practice, he has treated more than 40,000 patients across Central and South Texas.
His clinical work today centers on conservative, non-surgical care, with a 95% surgery-avoidance rate. When a patient genuinely needs bunion surgery, Dr. Henry tells them directly — and refers them to a surgeon he trusts personally.
What Your First Visit Looks Like
About an hour. Here’s what happens specifically for a bunion evaluation.
We listen first. How long you’ve had it. Whether it runs in your family. What pain you’re having and what’s changed in your life because of it. What you’ve already tried, and what you’ve been told by other doctors.
We perform a focused biomechanical examination. Foot and ankle range of motion, first-ray mobility, muscle testing, structural assessment of the foot off the ground. We check the great toe joint specifically — range of motion, crepitus, tenderness — to assess how much joint wear has already occurred.
We take weight-bearing digital X-rays in office. The way your bones align under your own body weight tells us things a non-weight-bearing image never could. We measure your hallux valgus angle, your intermetatarsal angle, and the joint surface itself. You see the images on screen with us, and we explain what we find in plain language.
Where appropriate, we use live diagnostic ultrasound to look at the soft tissue around the joint — bursa, capsule, tendons. Visible, immediately.
We perform a tape test on the bunion itself. The tape is diagnostic — how well it relieves your pain predicts how well you’ll respond to a custom orthotic protocol. It’s also therapeutic. Many patients walk out of their first visit with substantially less pain than they walked in with.
We give you our honest assessment, out loud. Surgery is rarely Plan A here — and for bunions specifically, it’s almost never Plan A, B, or C. On the rare occasion we genuinely believe surgery is the right answer for you, we’ll tell you directly, and if you’d like, we’ll refer you to a surgeon we trust. Far more often, we’ll show you the path that gets you better without it — and arrange a follow-up to see how you’ve responded to the taping and refine the plan from there.
About Bunion Surgery (What You’re Actually Signing Up For)
If you’ve been told you need bunion surgery, you should understand exactly what that means before you sign the consent form. Most patients don’t.
Bunion surgery is not a single procedure. There are essentially four levels of correction, ranging from minor to extensive. Which one you need depends on the severity of the deformity, the joint condition, and the surgeon’s preference.
Level 1: Simple Bumpectomy (McBride Bunionectomy)
Just shaves the prominence of bone on the inside of the foot. Doesn’t realign anything. Recurrence is common because the underlying mechanics that caused the bunion haven’t been addressed.
Level 2: Distal Osteotomy (Austin Bunionectomy)
Bumpectomy plus a V-shaped cut into the head of the first metatarsal to realign the joint. Held together with a pin or screw — sometimes absorbable, sometimes metal. Several weeks in a CAM boot. (The procedure is named for Dale Austin, DPM, who developed it. Not the city — though we wish.)
Level 3: Proximal or Base Osteotomy (Sometimes With First Metatarsal-Cuneiform Fusion / Lapidus)
Bumpectomy, joint realignment, plus a cut at the base of the metatarsal — or fusion of the joint at the base of the metatarsal. Metal plates and screws. Six to twelve weeks of immobilization.
Level 4: Joint Procedures for Advanced Disease
When the great toe joint has progressed to severe arthritis, the surgery is no longer just about straightening the toe — it’s about salvaging or replacing the joint. Implants, fusions (which permanently eliminate motion of the joint), or joint revisions.
A Few Things Every Patient Considering Bunion Surgery Should Know
You will have visible scars. At least one or two, usually on the top or side of the foot. They can rub against shoes and cause irritation for months — sometimes permanently. Most surgeons don’t mention this clearly during the consultation.
Bunions are notorious for recurring after surgery. Recurrence rates in the published literature range from 5% to 15% over ten years, and considerably higher for severe deformities or in patients who don’t address the underlying biomechanics afterward. Many surgeons plan their first bunionectomy with the assumption that a second surgery may be needed years later. The reimbursement model frankly doesn’t penalize them for this. You will need orthotics after surgery to prevent recurrence anyway — which is the central irony of this entire field of medicine.
About minimally invasive surgery (MIS) for bunions. This is being marketed aggressively right now. Smaller incisions, faster recovery, less visible scarring. The marketing is compelling. The literature is more complicated. MIS bunion surgery has a steep, well-documented learning curve — surgeons performing their first 50 procedures have nearly twice the complication rate of experienced ones. The visualization is fluoroscopic rather than direct, meaning the surgeon cannot directly see the small blood vessels and nerves they’re working around. There are also unique MIS-specific complications that don’t exist in open surgery — including skin burns from the high-speed burr (reported in 0–13% of cases in some studies), hardware displacement, and certain bone fracture patterns. In experienced hands, modern MIS techniques can be a reasonable choice for some patients. The question is whether the surgeon recommending it to you has done enough of these to be one of those experienced hands — or whether you’re paying to be part of someone’s learning curve. Dr. Henry has performed minimally invasive procedures for over four decades on conditions where the anatomy supports it — heel spurs, plantar fasciotomies, Morton’s neuroma releases — but does not perform MIS for bunion correction, because the complex anatomy of the first ray, in his judgment, does not lend itself reliably to operating without direct visualization.
About cosmetic bunion surgery. Some patients aren’t in pain — they just don’t like how their foot looks. Surgery for a painless bunion is generally inappropriate. A bunion that doesn’t hurt and is still progressing slowly is a candidate for orthotics, not for an operation that carries real risk of permanent scarring, joint stiffness, recurrence, and the chance of being worse off than you started.
The right time to operate on a bunion is when conservative care has been genuinely tried and isn’t enough — not when it hasn’t been tried at all.
Who We Treat
Patients come to us from across the Highland Lakes — Marble Falls, Kingsland, Burnet, Horseshoe Bay, Granite Shoals, Cottonwood Shores — and from across Hill Country, often specifically because they’ve been told they need bunion surgery and they’re not ready to accept that answer without a real second opinion.
A common story we hear: “My mother had bunions. My sisters have bunions. I figured this was just normal — until my second toe started hurting too.” If that sounds familiar, you’re not unusual. You’re not stuck either.
What Our Patients Say
“My mother had bunion surgery in her seventies. It was a disaster — she was in a boot for months and the bunion came back within five years. When my own bunions started hurting, I told my husband I would do anything to avoid surgery. Dr. Henry made me orthotics and showed me which shoes to wear. Two years later I’m walking three miles a day with no pain and my bunion looks the same as it did when I started. I’m so glad I came here first.”
— Margaret W., Burnet“I’d been to two other podiatrists and both told me I’d need surgery for both feet. The recovery time was going to be six months total and I didn’t want to lose the year. Dr. Henry was the first one to actually examine how my foot was loading. He explained why my bunions had formed and exactly what he could and couldn’t do for me. He was honest — he told me my bunions wouldn’t get smaller. But the pain went away within a few weeks of getting his orthotics, and a year later I haven’t had the surgery.”
— Joan T., Horseshoe Bay“My right toe was leaning so far over my second toe that I couldn’t wear closed shoes anymore. My family doctor sent me to a foot surgeon who scheduled me for the operation right away. My daughter convinced me to get a second opinion before signing anything. Dr. Henry took an hour with me, took new X-rays, and laid out a completely different plan. The taping he did at the first visit gave me more relief than the cortisone shot the other doctor had given me. Eight months in, I’ve cancelled the surgery.”
— Patricia L., SpicewoodCommon Questions About Bunions
Are bunions hereditary?
The bunion itself isn’t hereditary, but the foot mechanics that lead to one are. If your mother and sisters all have bunions, you’ve inherited a foot type — usually one that pronates excessively — that allows the first and second metatarsals to spread apart over time. The deformity develops slowly and is often visibly worse after pregnancy, particularly a second pregnancy, because the same hormones that loosen pelvic ligaments for childbirth also loosen the ligaments of the feet.
Can custom orthotics actually shrink a bunion?
No. Once the bone has shifted, no non-surgical treatment will move it back. What custom orthotics can do — and do reliably for the great majority of our patients — is eliminate the pain, halt the progression, prevent the cascade to second-toe hammertoe and great-toe-joint arthritis, and keep you out of the operating room. The bunion you walk in with is generally the bunion you keep — but it doesn’t have to hurt, and it doesn’t have to keep growing.
I have bunions but they don’t hurt. Should I still come in?
Yes — particularly if they’re getting visibly larger. A painless bunion that’s still progressing is exactly the kind of patient where conservative care has the most to offer. Custom orthotics worn at least half the time will usually halt progression entirely. Treating a bunion early protects you from the harder problems that come later: arthritis in the joint, a buckling second toe, and a much more involved surgery if the deformity becomes severe enough that surgery is genuinely needed.
What about bunion surgery — when is it actually the right answer?
Surgery is appropriate for severe deformity that hasn’t responded to genuine conservative care, for advanced great-toe-joint arthritis that’s limiting your function, and occasionally for rapidly progressing bunions where waiting would mean a much more involved procedure later. It’s not appropriate for cosmetic concerns alone, for painless bunions, or for patients who haven’t first had a real, sustained, expert attempt at non-surgical resolution. When surgery is genuinely the right answer, Dr. Henry will tell you directly and refer you to a surgeon he trusts.
I’m pregnant and noticed my bunion getting worse. What can I do?
This is one of the most underappreciated moments in bunion care. Pregnancy hormones loosen the foot’s ligaments along with the pelvis, and bunions that were stable can progress rapidly during and after pregnancy — particularly during a second pregnancy. Wearing prescription orthotics during pregnancy can substantially slow that progression. If your bunion has noticeably changed during pregnancy, schedule an evaluation. The earlier we intervene, the more we can prevent.